
Translate this page into:
Primary Endobronchial Conventional Chondrosarcoma Right Lung Upper Lobe: A Case Report and Literature Review


*Corresponding author: Prashant Gupta, Department of Surgical Oncology, Command Hospital (Eastern Command), Kolkata, West Bengal, India. drprashant42@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta P, Jaiswal P, Murthy HS, Bhatia JK. Primary endobronchial conventional chondrosarcoma right lung upper lobe: A case report and literature review. Indian Cancer Awareness J. 2024;3:22-6. doi: 10.25259/ICAJ_13_2023
Abstract
Primary endobronchial chondrosarcoma is extremely rare and hardly reported while reported chondrosarcomas of primary lung origin are rare with most literature coming from a series of case reports and small case series. These tumours can present as centrally located masses and therefore, require extensive workup to exclude alternative aetiology and to confirm diagnosis. Literature review revealed only four reports of primary endobronchial and 29 primary pulmonary chondrosarcoma cases, excluding the current report. We present a rare case of biopsy-proven non-metastatic primary endobronchial conventional chondrosarcoma of the right upper lobar bronchus extending into the right main bronchus managed with technically challenging sleeve bilobectomy of right upper and middle lobes and a viable anastomosis of lower lobe bronchus with the right main bronchus stump and thus, prevented a pneumonectomy. Final histopathology confirmed the diagnosis. Thus, these tumours are difficult to diagnose and challenging to manage and need more data in future to establish protocols.
Keywords
Primary endobronchial
Pulmonary
Conventional
Chondrosarcoma

INTRODUCTION
Chondrosarcomas of primary lung origin is an extremely rare pathology with most descriptions coming from a series of case reports and small case series with even fewer reports of tracheobronchial chondrosarcomas. These tumours can present as centrally located, parenchymal masses. Diagnosis requires extensive workup to exclude alternative aetiology and to confirm diagnosis. To date, only 29 cases of lung and four of bronchial origin, not including the present study, of this pathology have been reported.[1-6] Herein, we present a rare case with biopsy-proven non-metastatic primary conventional endobronchial chondrosarcoma of the right upper lobe (RUL) managed with challenging sleeve bilobectomy.
CASE REPORT
A 52-year-old reformed smoker and hypertensive male presented to surgical oncology clinic for non-productive cough of 6-month duration. On physical examination, the patient was detected with reduced breath sounds in the right upper zone of chest with mild expiratory wheezing on the right side. Relevant laboratory results were unremarkable.
Evaluation with chest X-ray revealed a homogeneous opacity in the upper zone of the right hemithorax [Figure 1a] which prompted further evaluation with contrast-enhanced computed tomography (CT) revealing a 13 × 8 × 9 cm mass in apical and posterior segment of the upper lobe of the right lung with few foci of calcifications within. The lesion was close to the right wall of trachea with an abrupt cutoff of the right main bronchus at the axial level of dorsal vertebra4-5 and collapse of RUL [Figures 1b and c]. Few discrete lymph nodes were present in prevascular, pretracheal, right paratracheal and aorto-pulmonary window stations with largest being only 7 mm. Bronchoscopy revealed an endobronchial mass partially occluding the right main bronchus, originating from RUL bronchus completely occluding its lumen [Figure 1d]; however, scope could be negotiated ahead finding normal openings of right middle lobe (RML) and right lower lobe (RLL) bronchi. Bilateral vocal cords were normal.
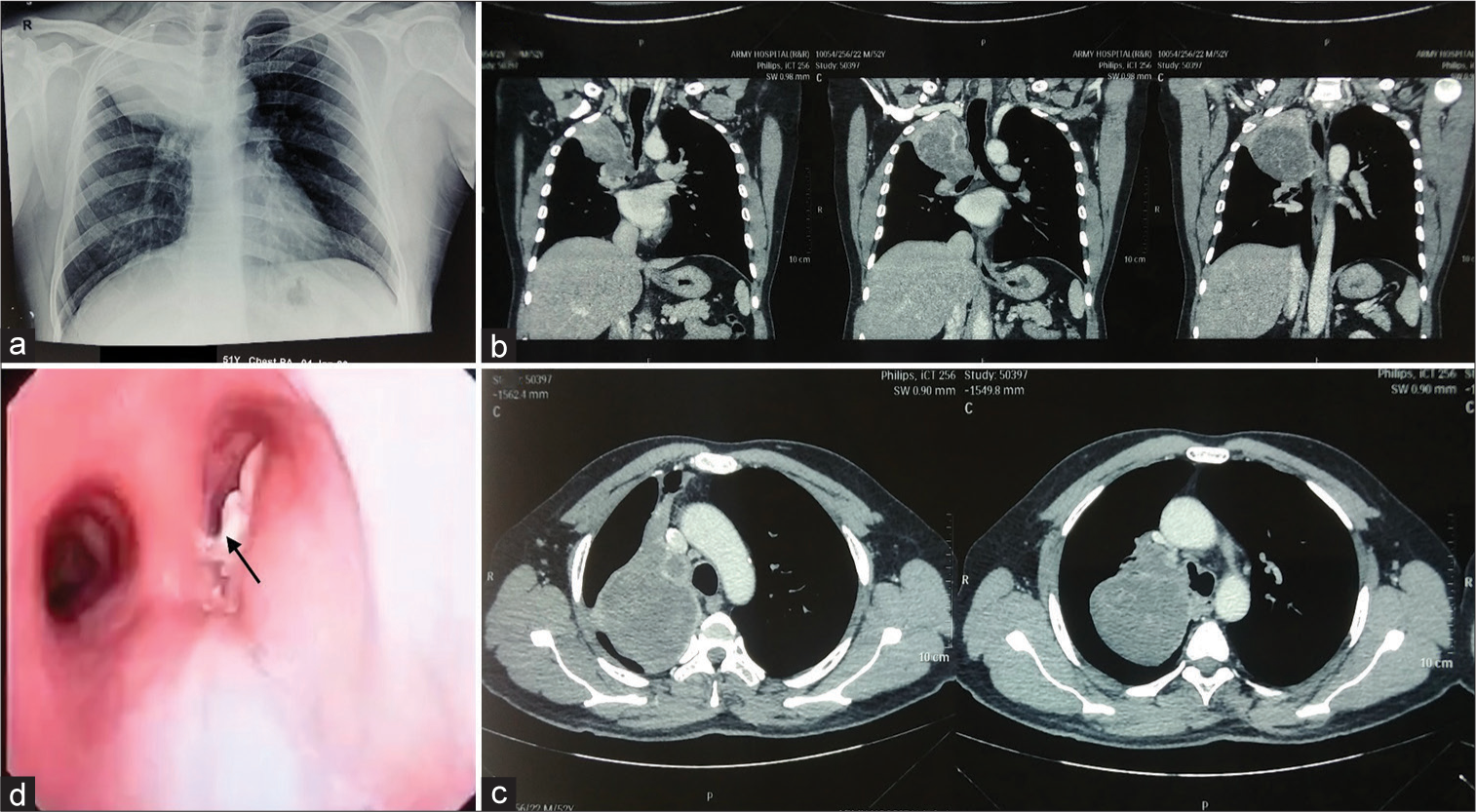
- Pre-operative imaging. (a) Chest X-ray showing homogeneous opacity upper zone right hemithorax. (b), (c) Contrast-enhanced computed tomography chest coronal and axial views showing large heterogeneously enhancing mass right lung upper lobe infiltrating main bronchus with luminal compromise. (d) Bronchoscopy showing proliferative lesion right main bronchus (arrow) opposite to carina with negotiable partial occlusion and patent left main bronchus.
18-Fluoro-deoxy-glucose positron emission tomography-computed tomography scan did not reveal any avid mediastinal lymph nodes or any other lesion elsewhere in the body excluding the possibility of Carney triad too. Therefore, a CT-guided biopsy was conducted from the lung mass which indicated conventional chondrosarcoma of lung, positive for Vimentin on immuno-histo-chemistry but negative for Cytokeratin (CK), Calponin and isocitrate dehydrogenase 1. Patient was, therefore, diagnosed as non-metastatic primary chondrosarcoma of lung and planned for surgical resection. Hence, in preparation for surgery, pulmonary function tests were done which were indicative of mild restriction only. Further evaluation with Diffusion capacity of lungs for carbon mono-oxide (DLCO) showed 86% carbon monoxide diffusion and ventilation-perfusion scan was suggestive of 64% of the left lung and 36% of the right lung perfusion in differential lung function. Estimated residual lung function post-right upper lobectomy forced expiratory volume in 1 second was 2.55 L/s and post-pneumonectomy was 1.86 L/s. He was, thus, counselled for sleeve lobectomy with possibility of conversion to pneumonectomy and its associated complications in view of possible involvement of the right main bronchus.
An exploratory right posterolateral thoracotomy revealed a mass of about 12 cm in size involving the RUL with adhesion to RML, poorly defined horizontal fissure but well defined oblique fissure [Figures 2a and b]. Lower lobe, chest wall and mediastinum were free from the lesion with no pleural surface deposits. After posterior dissection at the hilum, the right main bronchus was isolated and looped followed by lower lobe bronchus [Figure 2c] but the middle lobe bronchus was found to be involved by the tumour. The lesion was found to be in the right main bronchus about 2.5 cm distal to carina. Hence, the right main bronchus was incised open proximal to the lesion with an intent of sleeve upper lobectomy [Figure 2d]. The middle lobe bronchus being involved led to sleeve bilobectomy including upper and middle lobes which were completed with careful dissection and stapling of the upper and middle lobe branches of pulmonary artery and vein with resection of upper and middle lobe bronchi taking tumour-free margins all around confirmed on contemporary frozen section. The lower lobe bronchus was then anastomosed with the right main bronchus stump using interrupted polydioxanone suture 3-0 sutures [Figures 2e and f] and leak test with normal saline confirmed negative with good aeration of the lower lobe. Specimen was examined [Figure 2g] and thoracotomy closure was done over an intercostal drainage tube and after extubation patient was shifted to intensive care unit in stable condition for observation. Post-operative chest X-ray showed good expansion of the RLL with no air leak [Figure 2h].
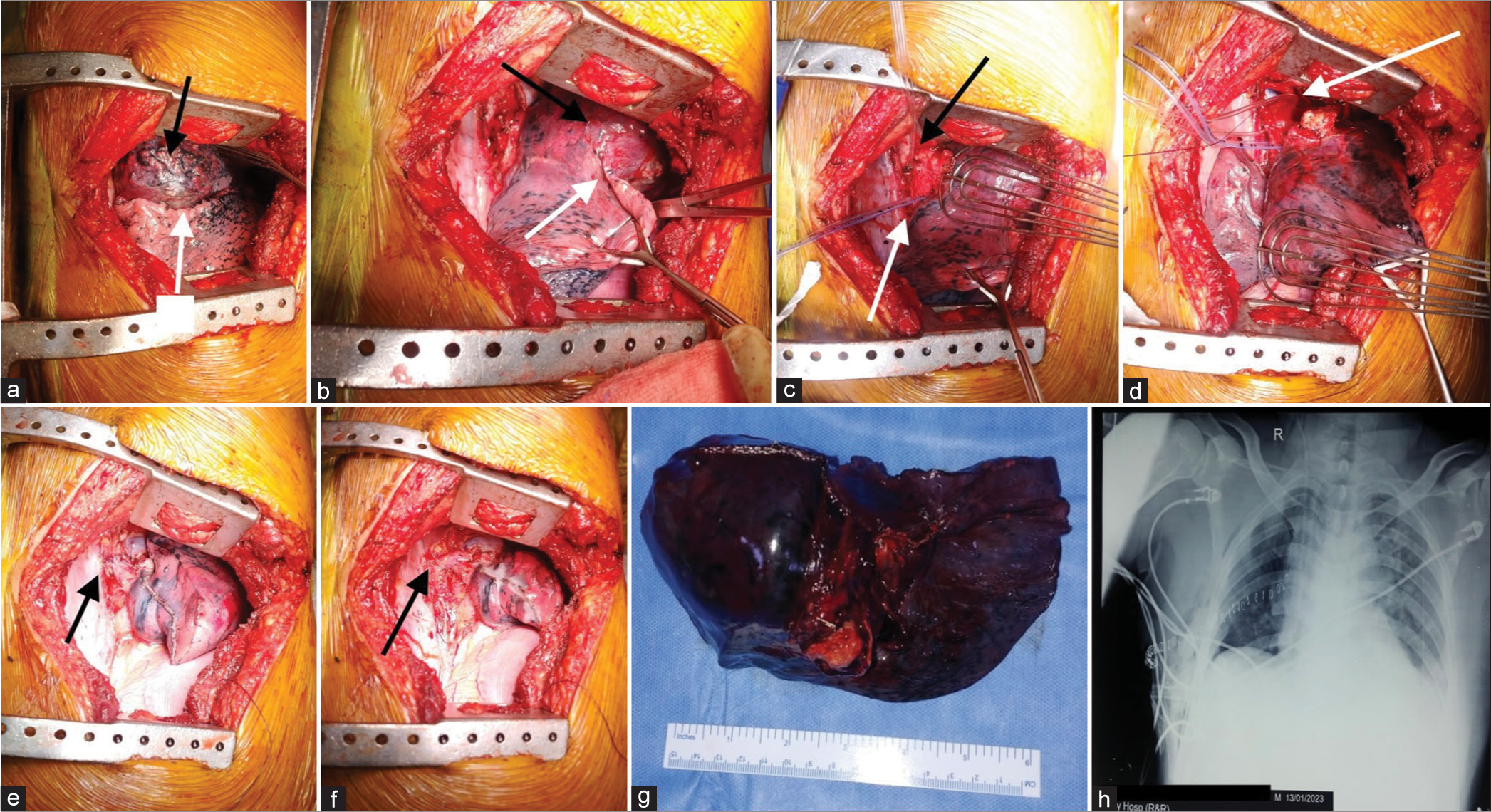
- Intraoperative images. (a and b) Mass in the right upper lobe (black arrows) with well-defined oblique fissure (white arrows). (c) Right main (black arrow) and lower lobe bronchus (white arrow) looped. (d) Right main bronchus was cut open above the lesion with gross negative margin and intact membranous portion (arrow). (e and f), Completed lower lobe bronchus to main bronchus stump anastomosis (arrow) covered with mediastinal pleural patch (arrows). (g) Resected specimen with right upper and middle lobe and growth at the bronchus. (h) Post-operative chest X-ray showed adequately expanded right lower lobe.
Histopathologic examination revealed 8 cm size unifocal tumour having multinodular architecture with fibrous septa dividing the tumour in pools of abundant chondromyxoid matrix containing tumour cells [Figure 3a]. Spindle cell differentiation was noted and stroma was hypovascular. Abundant cartilaginous matrix with chondrocytes embedded in lacunae was seen. Tumour was arranged in nested pattern with intervening fibrovascular septae, multinucleation and brisk mitosis were seen in tumour cells [Figures 3b and c]. No visceral pleural, lymphovascular or perineural invasion was identified. Immunohistochemistry – epithelial membrane antigen – focal positive, S-100 positive and PanCK, CD99, CD56 and Synaptophysin negative [Figures 3d-i] thus clinching final diagnosis of high-grade conventional chondrosarcoma with stage pT1N0 and tumour-free margins.
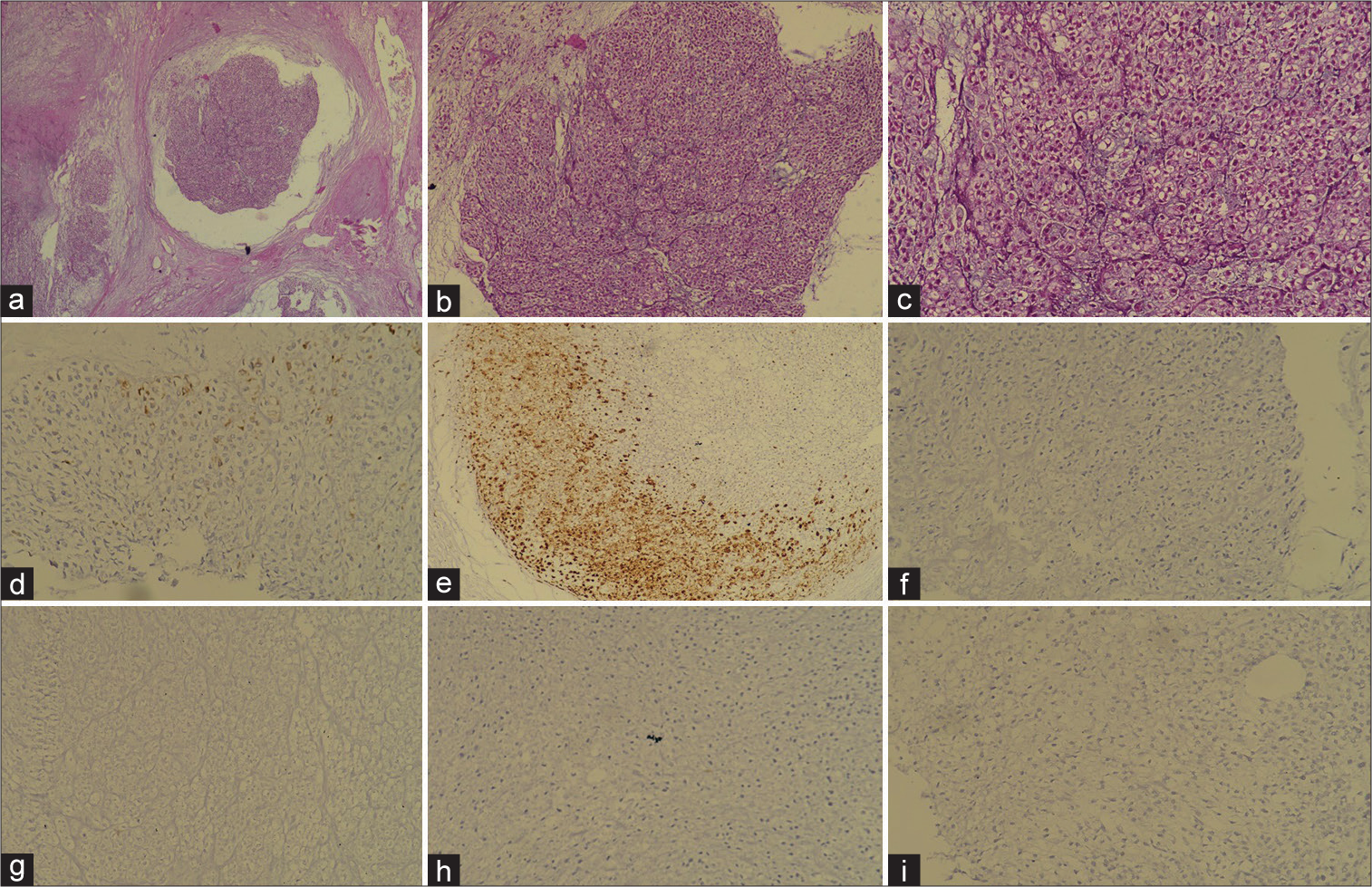
- Histopathology images. (a) Haematoxylin and eosin (H&E) stain with ×10 magnification showing tumour in nested pattern with chondromyxoid stoma. (b), (c) H&E stain with ×20 magnification showing multinucleation and brisk mitosis. (d) EMA focal positive. (e) S-100 positive. (f) Pan-CK negative. (g) CD99 negative. (h) CD56 negative. (i) Synaptophysin negative.
DISCUSSION
Primary bronchial and lung chondrosarcomas are extremely rare with descriptions coming almost exclusively from case reports.[1,2] while cases reported as endobronchial chondrosarcomas are almost non-existent. PubMed, Researchgate and Google searches using terms ‘primary endobronchial chondrosarcoma’ OR ‘primary bronchial chondrosarcoma’ OR ‘primary chondrosarcoma of bronchus’ OR ‘chondrosarcoma bronchus’ OR ‘bronchial chondrosarcoma’ OR ‘conventional chondrosarcoma bronchus’ OR ‘primary conventional endobronchial chondrosarcoma’ yielded only four case reports.[3-6] Hence, their incidence is difficult to estimate as these tumours are frequently misdiagnosed, requiring an extensive clinical history and diagnostic workup to exclude primary origin elsewhere and thus, they may be underreported in the literature.
Patients with pulmonary chondrosarcomas present with symptomatic pulmonary obstruction, dyspnoea and chest pain. To diagnose a lung primary, a detailed clinical history and appropriate imaging are essential to exclude the following criteria: History of thoracic cage neoplasm, skeletal neoplasms, limb amputation and teratoma.[7] Furthermore, Carney triad (pulmonary chondroma along with gastrointestinal stromal tumour and extra-adrenal paragangliomas) should be excluded from the study.
CT scans that demonstrate a well-demarcated, centrally located mass with calcifications may be indicative of pulmonary chondrosarcoma, though the presence of calcifications is disputed[7] and thus, should be a differential diagnosis of patients with similar presentation as this case. Histologically, these tumours are characterised by ill-defined lobules containing differentiated hyaline cartilage with plump nuclei, hyperchromasia, binucleation and coarse chromatin.[7] Sometimes basophilic myxoid stroma with focal areas of hyaline cartilage may also be seen.[7] Immunohistochemical studies are negative for keratin, CD31 and desmin and are S-100 positive.
Complete surgical resection of the tumour is recommended as malignant cartilage with mixed epithelial/mesenchymal neoplasms may be observed. Complete resection will prevent misdiagnosis based on improper biopsy specimen as teratomas may resemble pulmonary chondrosarcoma from inaccuracy of biopsy location.[7] These tumours may metastasize to distant sites such as the contralateral lung, skull and kidneys, where adjuvant chemotherapy may be beneficial.
Further reporting, investigation and study of the radiological findings in such cases of extraskeletal primary chondrosarcomas and reported outcomes are, therefore, needed to establish reliable diagnostic criteria and treatment recommendations.
CONCLUSION
Extraskeletal chondrosarcomas are rare with scarce literature and primary endobronchial conventional chondrosarcomas being an extremely uncommon extraskeletal site needs detailed evaluation to rule out other primary site and definitive surgical management preventing a pneumonectomy.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Primary pulmonary chondrosarcoma: A case report and literature review. J Clin Imaging Sci. 2020;10:3.
- [CrossRef] [PubMed] [Google Scholar]
- Chondrosarcoma of the bronchus: Report of a case with resection and review of the literature. Chest J. 1983;84:224-6.
- [CrossRef] [Google Scholar]
- Primary chondrosarcoma of the left inferior lobar bronchus. Respiration. 1989;56:241-4.
- [CrossRef] [PubMed] [Google Scholar]
- Chondrosarcoma of the lobar bronchus with prolonged postoperative survival. Eur Respir J. 1994;7:1537-8.
- [CrossRef] [PubMed] [Google Scholar]
- Primary pulmonary chondrosarcomas: A clinicopathologic study of 4 cases. Hum Pathol. 2011;42:1629-34.
- [CrossRef] [PubMed] [Google Scholar]




